STOMA: FINALLY EXPLAINED (Part 1)
In the previous article, we demystified the different types of stomata: urostomy, colostomy and ileostomy. Today, you will learn about why and how a stoma is made. Usually, if you have to undergo this type of surgery, an ET nurse or another key person must explain to you what the surgery is. Don’t hesitate to ask questions to your doctor and nursing staff. We’re here to answer them, and this can help you be more relaxed before surgery. What I’m describing in this article does not apply to every single case. There will always be isolated cases where the operation will be different. This article will be divided into two parts, and this was the first one.
First, a radical cystectomy can be performed to make a urostomy. For men, this means completely removing the bladder, prostate and seminal vesicles. Then, surgeons create an ileal conduit by taking a short segment of the ileum (part of the intestine) and connecting one end to the stoma located on the abdomen. Ureters are connected to the ileal conduit. The two other segments in your intestine are connected together. A urostomy made like this usually is permanent. In some centres, certain surgeons offer bladder reconstruction if a patient’s health allows it.
People suffering from uterine, vaginal, cervical, vulvar or prostate cancer, or anal cancer that spread to surrounding organs may require posterior, anterior or total pelvic exenteration. Depending on the cancer’s severity, surgeons can remove the womb, cervix, ovaries, fallopian tubes, prostate, seminal vesicules, rectum, bladder and part of or the entire vagina. Total pelvic exenteration means removing the bladder and rectum. This type of surgery can lead to a colostomy and a permanent urostomy, depending on the case and the patient’s clinical history.
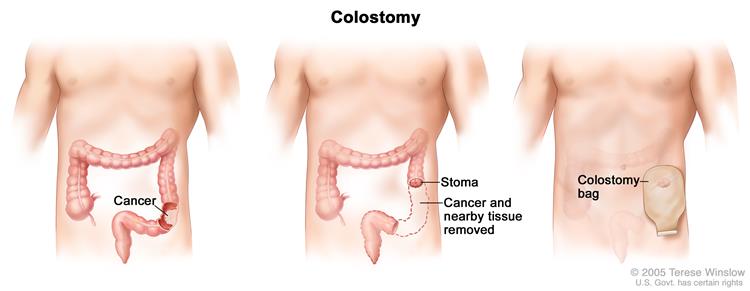
The Hartmann’s procedure is usually performed during emergencies where a patient’s condition is unstable and the anastomosis between two parts of the intestine is not possible. The procedure consists of removing the diseased part of the colon and performing a terminal colostomy. The other part of the intestine is closed and remains in place, in case an anastomosis can be performed once the colon is healed. The colostomy is either permanent or temporary, depending on the medical diagnosis. The part of the colon remaining in your body will continue to produce mucus. It will be expelled the same way when you defecate.
Proctocolectomy is the complete removal of the large intestine, rectum and anus. The anus is closed at the perianal level, and an ileostomy is performed in the lower right quadrant, at the end of the ileum. Some people may have a proctocolectomy with an ileo-anal pouch, which consists of two surgeries. The first one consists of complete resection of the large intestine without removing the sphincters. The second one consists of making the “pouch”: part of the ileum is placed in a “J” shape and is anastomosed to the dentate line and the skin. It’s a curative surgery for ulcerative colitis and familial adenomatous polyposis.
This concludes the first and more complex part of this article about surgical procedures.